Beware of Dentures

It may surprise you, but I would not wish a denture on my worst enemy. This may seem hyperbolic, but it is accurate-I wish good health over less-than-perfect treatment for everyone. I make them, but I warn patients that as much as they can replace teeth and improve appearances and chewing, they have many pitfalls. I warn patients that they may appreciate appearing as if they have all of their teeth, but there will be a host of problems with them. In short, the best dentures in the world will still have numerous problems; they may marginally function as natural teeth. As patients age, they usually become less functional over time. Many times, late in life, they can no longer be tolerated while eating and may only serve for cosmetic appearances, if even that. In short, dentures always come with a dose of suffering; sometimes minimal, sometimes horrific. In the end most patients with dentures learn to live with them. All of them wish they had real teeth, however.
Luckily, we have implants that can keep most people away from dentures, but they can be quite expensive and unattainable for people with limited resources. This post will cover dentures' good, bad, and ugly aspects. Hopefully, it will serve as a warning to take care of yourself and never need them.
What Are Dentures?
Dentures are removable replacements of one or more teeth. The technical term for a denture is a removable prosthesis. The meaning of a prosthesis is An artificial device used to replace a missing body part, such as a limb, tooth, eye, or heart valve. 1 A prosthesis can also be called a prosthetic device. Dentists who specialize in placing them exclusively are called prosthodontists. Since dentures are common, most dentists can make them for you; prosthodontists are usually needed for complicated cases. Prosthetics can be fixed in place. Crowns, bridges, and dental implants are some examples. This post will only cover the removable ones.
Types of Dentures

Generally, dentures are categorized as partial or full. Full dentures replace an entire arch of teeth, whereas partial dentures replace one or more teeth and blend with the remaining natural teeth. Full dentures are usually plastic, although the teeth can be porcelain. The pink part of the denture that mimics the appearance of gums, known as the denture base, is exclusively made of plastic. The base of full dentures is usually rigid. Partial denture bases, on the other hand, can be acrylic or metal, rigid, or flexible. The portion of the gums that the denture rests on is called the residual ridge.
How Dentures Stay In

Full upper dentures need to cover the entire hard palate and a small portion of the soft palate to create suction to keep them in. Because they need to extend to the back of the palate, they are quite bulky. They may dislodge while eating or speaking if the suction is inadequate. Denture adhesives are over-the-counter products that temporarily glue the denture to the mouth's soft tissue to help them stay in place.
Partial dentures usually employ clasps that grab onto natural teeth to help retain them in the mouth. Partial dentures are usually more stable than full dentures, but only sometimes. The number of remaining teeth may limit how well they stay in. Also, the condition and shape of the teeth may limit retention.
Implants are sometimes used to house precision attachments that the denture can snap into. The implant is fixed to the jaw and contains one-half of the snap combination. The other half of the snap combination is on the underside of the denture. The denture is still considered removable but can be rigid while in place. Furthermore, because the denture covers the implant, it is called an overdenture.
Precision attachments don't need implants to be placed. The kind that looks like the implant-supported attachments can be placed in a natural tooth, but removing the nerve via a root canal is necessary. Alternatively, teeth can be covered with crowns that house precision attachments, usually on their sides.
Care of Dentures
Since dentures spend all day in the mouth, they are subject to plaque buildup and wear. They need to be taken out and brushed. Cleaning agents are available specifically for dentures, but antimicrobial soap can be used. Additionally, soaking them to remove stains and odor is recommended. Products are also available for soaking but won't substitute for brushing. Dentures should be taken to the dentist every six months for cleaning, inspection, and maintenance.
The Good

Dentures are cosmetic devices because they replace missing teeth that most patients find unsightly. They can help to chew to varying degrees, but it depends on help from the supporting tissues like gums and teeth. As mentioned before, attachments can be a big help. Additionally, they can maintain cheek and lip support for better appearance and function. They can help speech articulation, especially of F and TH sounds, especially when the upper anterior teeth are involved. They can psychologically boost patient confidence and mood due to normalizing appearance and function.
The Bad
Getting Used to Them: When new, patients need to accommodate to them. Their size will limit tongue and cheek mobility, affecting speech, chewing, and swallowing. They may place undue pressure on the gums and cause irritations. Speech, chewing, and swallowing improve quickly and naturally. However, lasting changes should be expected. The changes can be so severe that patients never fully accommodate to them, which causes functional and emotional problems.
Chewing: Patients can expect less ability to chew with dentures. Dentures with fewer teeth usually perform better, especially when clasps and attachments are involved. Full dentures that rest on the gums have much less chewing ability than natural teeth. Full upper dentures are more stable because they rest on the palate. But there is a catch-the salivary glands on the palate when covered, will cause the mouth to become dryer. Discomfort and irritation of the tissues can occur. Dry mouths are also much more prone to tooth decay.
Additionally, the taste of food can change. Conversely, lower full dentures are orders of magnitude less capable of functioning because they only have a small lower ridge to rest on. All full lower dentures are unstable unless they have precision attachments.
Speech: Since upper dentures usually rest on the palate, the tongue articulates S, T, L, and D sounds on the denture base instead of the palate, causing their sound to change. The changes can be minimal or drastic. Lower dentures cause fewer speech problems because lower teeth are not used for speech articulation.
F and V sounds may also change because the lower lip and the upper teeth must work together to achieve them. Alterations in the upper anterior teeth shape, length, and thickness will change speech dynamics. Additionally, escaping air during F and V sounds will change. The changes may be slight or drastic.
One final note on speech: Patients and those close to them will notice the changes more. Strangers and acquaintances may not even notice the difference, but the patient may suffer emotionally because they can be self-conscious.
Swallowing and Gagging: Similar to speech, swallowing can suffer. When we swallow, our tongue coordinates with the palate. Upper dentures that cover the palate will interfere. Full upper dentures cover the most palate, and partial dentures vary. The difficulty varies from patient to patient and is always worse while getting used to new dentures. Gagging is normal when dentures are new; most patients get over it quickly. Unfortunately, many patients never get over it. Patients with severe gag reflexes either can't wear their dentures or need implants placed and/or the palatal portion of the denture removed. Without implants, removing the palatal coverage will destroy the denture's ability to stay affixed.
Hygiene: Dentures will coat with plaque just like real teeth and need brushing. They also develop stains and odor, which, as I mentioned, can be mitigated. While eating, food particles will lodge in areas around dentures. All dentures need to be removed after meals and cleaned, which is not always possible. With partial dentures, the natural teeth will become more prone to decay and gum disease due to food impaction and plaque buildup.
Wear, Bite Collapse, and Super-eruption: Dentures wear out. They wear more quickly when they function against natural teeth, especially crowned ones. As the plastic teeth wear, the opposing natural teeth will erupt further to maintain their articulation ability during chewing. Super-eruption is when natural teeth grow too far out of the gums. This condition presents severe problems with chewing. Super-erupted teeth are very complicated to treat, if they can be treated at all. Wear and super-eruption are good reasons to visit your dentist every six months. Unfortunately, the type of patients that are denture candidates only sometimes visit the dentist regularly. Since patients are usually unaware of super-eruption, it may be too late for a successful fix by the time they notice it.

Full dentures, singly or in pairs, also wear down. Super-eruption does not occur in these cases. Instead, the lower jaw closes farther as the wear increases. Eventually, the lower jaw can close farther than it is designed to. The patient will have a shorter face, and creases will appear in the corners of the mouth. We call this a collapsed bite. The joints will remodel and can become arthritic and painful.
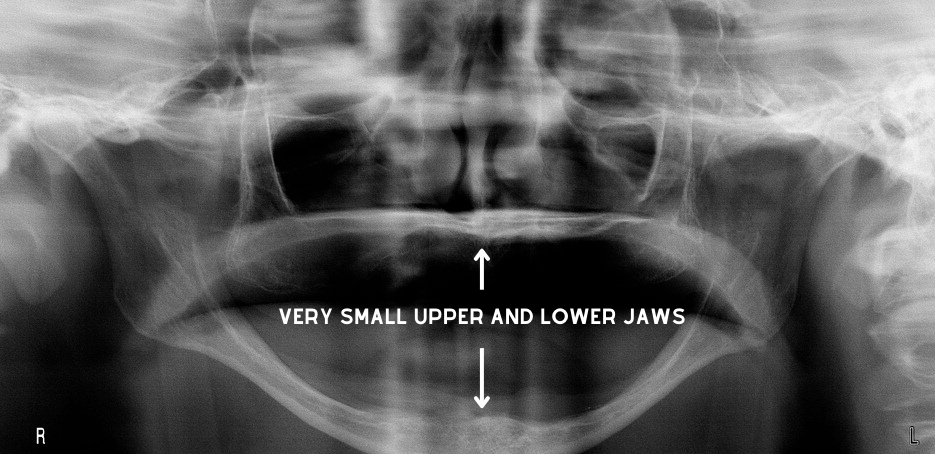
Shrinking Jaws: The jaws exist to hold natural teeth in place. Once teeth are gone, the body will not maintain the jaws. Bone will slowly disappear. The upper jaw residual ridge recedes posteriorly while the lower residual ridge moves anteriorly. Relining the denture base periodically helps keep the dentures fitting and functioning properly.
Eventually, patients will appear as if their lower jaw juts forward. The lower jaw (mandible) usually becomes so atrophic (small) that the lower denture cannot stay in place and becomes useless. I see this in most of my elderly patients. Implants can be a great solution, but they usually have a fixed income and can't afford the treatment.
Malnutrition, Starvation, and Shorter Life: I wrote in this post that the fewer teeth we have, the greater likelihood of malnutrition, disease, and early death. Once my patients reach the final stages of edentulism (no teeth), they are quite miserable. They universally regret losing their teeth. According to Denturewearers.com, up to 95% of patients may regret having their dentures. 2
While There is Still Time: Eating a nutrient-dense diet without processed carbs and seed oils prevents most health woes, including tooth decay and gum disease. If you are unwilling to do that, then brushing your teeth twice daily and flossing once is necessary. Toothpaste is very optional. Visit your dentist at least twice yearly, even if you have no teeth, especially if you have dentures.