Navigating the Shadows of Dental Fear: Understanding Phobias and Irrational Behaviors

In the quiet hum of a dental office, where the scent of clove and sterile tools fills the air, a hidden battle often unfolds—not against decay or infection, but against the invisible grip of fear. As a seasoned dentist performing thousands of procedures annually, I've witnessed firsthand how phobic behaviors transform routine visits into ordeals of anxiety and avoidance. Patients arrive trembling at the thought of pain that rarely materializes, only to delay treatments that could end their suffering swiftly. This paradox raises profound questions about human psychology: Why do some endure imagined terrors while neglecting real relief? Exploring fear, phobias, and irrationality reveals not just the quirks of dental dread, but broader insights into how we confront—or evade—the discomforts of life.

From my vantage point behind the mask, dental phobia isn't just an occasional quirk; it's a pervasive force affecting a significant portion of patients. Studies suggest that up to 20% of adults experience severe dental anxiety, with many avoiding care altogether until emergencies force their hand. I see this higher percentage of phobic behavior daily. Despite advancements in anesthesia and techniques that render most procedures virtually painless—think numbing gels, laser dentistry, and sedation options—patients often arrive with hearts racing and palms sweating over "potential" discomfort. It's baffling because, after years in the field, I'm acutely aware that the vast majority of treatments involve minimal to no pain. A simple filling or cleaning? Often less bothersome than a mosquito bite. Yet, the fear persists, amplified by outdated horror stories or childhood traumas.
But the irrationality extends beyond mere anticipation. Take the patient who calls in agony from a throbbing toothache, describing pain that disrupts sleep and meals. They book an urgent appointment, only to hesitate when I outline a straightforward root canal or extraction that could banish the torment within hours. "Can't we wait and see?" they plead, or "What if it hurts more?" Excuses pile up: work commitments, cost concerns, or vague hopes that antibiotics alone will suffice. I can't help but ponder: Why make the appointment at all? Did they seek validation for their pain, a diagnosis to rationalize their suffering, or perhaps a subconscious desire to confront the issue without fully committing? It's as if the fear of intervention outweighs the very pain they're enduring, turning logic on its head.
This pattern repeats with preventive care. Small issues—a tiny cavity or early gum inflammation—could be addressed affordably and painlessly if caught early. Instead, many let them fester. Months or years later, they return swollen, infected, and miserable, requiring extensive (and expensive) interventions like crowns, implants, or surgeries. The refrain is predictable: "See, that's why I don't come; it's always too expensive and painful. I hate dentists." It's a self-fulfilling prophecy, where avoidance breeds the very outcomes they dread. This blame-shifting underscores a deeper irrationality: projecting personal fears onto the provider while ignoring how procrastination escalates both costs and discomfort.
To understand this, we must dissect fear, phobias, and irrational behavior. Fear is a primal response, an evolutionary alarm system alerting us to threats. In dentistry, it might stem from real dangers like infection, but often it's misplaced—triggered by the unknown or sensory cues like the drill's whine. Phobias elevate this to an extreme, irrational level: an intense, persistent fear disproportionate to the actual risk. Dental phobia, or odontophobia, fits the DSM-5 criteria for specific phobias, involving avoidance, distress, and interference with daily life. Irrational behavior here manifests as cognitive distortions—catastrophizing minor sensations into agony, or all-or-nothing thinking where one bad experience taints all future ones.
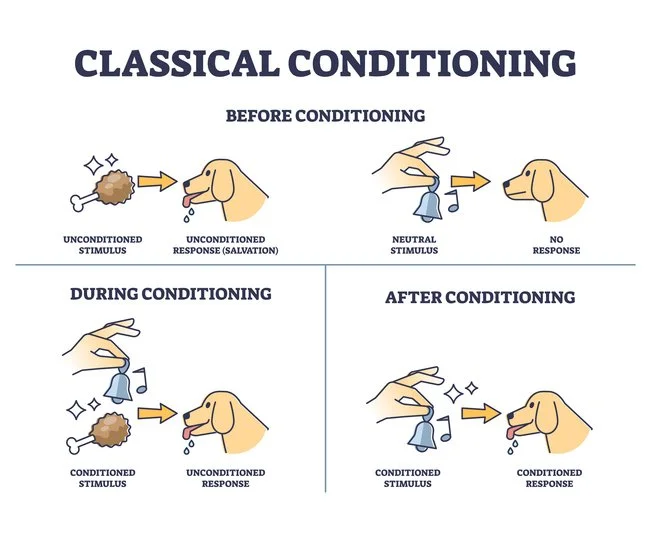
Theories abound to explain these phenomena. Behaviorally, classical conditioning plays a key role, per Pavlov's model: A painful childhood filling pairs the dental chair with trauma, conditioning future anxiety. Operant conditioning reinforces avoidance; skipping appointments temporarily reduces fear, strengthening the habit. Cognitively, Aaron Beck's theory highlights negative schemas—deep-seated beliefs, such as "Dentists cause pain," that filter experiences in biased ways. From a neurobiological angle, the amygdala's hyperactivity in phobics amplifies threat perception, while low GABA levels might reduce inhibition of fear responses. Evolutionary psychology suggests that dental fears tap into ancestral vulnerabilities: sharp tools evoke predation fears, and the loss of control in the chair mirrors helplessness. Social learning theory, via Bandura, posits that observing others' dread—through family stories or media—models phobic behavior. Finally, attachment theory links it to early relationships; insecure attachments might foster mistrust in authority figures like dentists.
Overcoming these fears and phobias requires multifaceted strategies. Cognitive Behavioral Therapy (CBT) is the gold standard, challenging irrational thoughts through exposure. Graduated exposure starts small—visiting the office without treatment—building to full procedures, desensitizing the fear response. Mindfulness and relaxation techniques, like deep breathing or progressive muscle relaxation, calm the autonomic nervous system during visits. Pharmacological aids, such as anti-anxiety meds or nitrous oxide, provide a bridge for severe cases. Hypnotherapy reframes subconscious associations, while virtual reality simulations allow safe practice. For dentists, building trust is crucial: Clear communication, empathy, and patient-centered approaches—like explaining each step or offering breaks—demystify the process. Encouraging early, positive experiences in children prevents phobia onset. Self-help tools, apps with guided imagery, or support groups normalize fears, empowering individuals to reframe dentistry as maintenance, not menace.

Yet, why do some handle immense fear and pain rationally, while others crumble under what feels like "1000 paper cuts"—minor stressors amplified into crises? Resilience varies due to factors like genetics, upbringing, and personality. High neuroticism, per the Big Five model, correlates with heightened sensitivity to threats, making every twinge a catastrophe. Conversely, those with high conscientiousness or optimism approach challenges logically, viewing pain as temporary. Pain tolerance theories, such as the Gate Control Theory by Melzack and Wall, explain how psychological factors modulate sensory input; focused attention or a positive mindset "closes the gate" to pain signals. Stoic individuals, perhaps shaped by adversity, employ rational coping—breaking problems into steps, weighing pros/cons—versus emotional reactors who spiral into avoidance. Cultural influences matter; societies that value endurance (e.g., military training) foster a rational approach to fear. Neuroplasticity allows rewiring through therapy, but early life stress can entrench hypersensitivity, turning paper cuts into wounds.
In essence, dental phobia illuminates broader human frailties: Our brains, wired for survival, sometimes misfire in modern contexts. By understanding theories and embracing interventions, we can transform dread into a manageable routine. As a dentist, I urge: Face the fear early; the relief on the other side is profound. Don't let irrational shadows dictate your health—step into the light, one appointment at a time.