My Face Fix So Far

I have written numerous posts on the plight of our small jaws over the years. So I thought it might be a good idea to share my story, and what I have done about it. I’m sure many people may look at my teeth and assume I’m in “good shape”. Just because teeth appear straight does not mean all is well. Dentists should be aware of your entire craniofacial respiratory system, which means paying attention to where your jaws are in relation to the rest of your face, especially your nose and pharynx.
Maternal Cigarette Smoking
Several papers dating back to 1954 have noted that the uterus is a low oxygen environment, and lowering the oxygen any further will retard fetal development, including the jaw. 1,2 My colleague Dr. Kevin Boyd is conducting research at the University of Pennsylvania on older skulls and has found that lowering the oxygen in utero results in smaller jaws. Watch him talk about it here.

Smoking causes a lower oxygen environment in utero which can cause jaws to underdevelop. Unfortunately, my mother was pregnant with me in 1961 when they did not discourage smoking while pregnant. As a result, her smoking may have led to my jaws being too small. Other maternal problems that can lead to lower oxygen environments for developing babies are apneas, sinus, tonsil, adenoid problems, allergies, and more.
Infant Formula and Breastfeeding

Back when I was an infant, breastfeeding was discouraged. As a result, I missed out on two crucial facial growth and development factors. The first is human breast milk. As I often say, human breast milk is the perfect infant food. Breastfed infants have a different growth pattern than formula-fed infants, and it is regarded as optimal. Breastfed infants increase weight, length, and BMI during the first three months of life and then have a slower growth velocity up to 12 months. They also have a higher accumulation of fat during early infancy. 3 The second critical factor for proper craniofacial development is suckling on a human nipple. In addition to the multiple advantages that mother's milk offers newborns, breastfeeding also helps correct craniofacial development for the incisor position and the mandible's vertical and sagittal relations with upper maxillary and cranial basis. 4
Weaning and Food Consistency

Premature introduction to spoon-feeding introduces improper swallowing, another cause of facial malformations. The transition to normal swallowing takes place at twelve to eighteen months. But even today, most parents introduce mushy foods around one year of age or sooner. Early spoon-feeding can prevent normal swallowing; poor swallowing can trigger undesirable facial growth. 5 The cure for this problem is simple, chew hard foods. I like all of us, was spoon-fed too early, and ate a typical soft diet growing up.
Tonsils and Adenoids

When I was an infant and toddler, having one's tonsils and adenoids removed was a rite of passage. Between 1915 and the 1960s, their removal was the most frequently performed surgical procedure in the United States. The tonsils were blamed as "portals of infection," their removal became the standard. 6 I had mine out (and both of my brothers did too) because doctors thought they were the source of my recurrent ear infections. My tonsils and adenoid removal may have benefitted me because they can obstruct the airway when swollen and enlarged. Their removal gave me more room to breathe in my nasopharynx.
Chronic Sinusitis and Deviated Septum

My sinuses were chronically infected for years, making it very difficult to breathe through my nose. Additionally, I had a deviated septum that occluded the nasal passages and made breathing even more difficult. I had both issues corrected with one surgery many years ago and had untold amounts of relief. I found it infinitely easier to breathe after the surgery. My difficulties breathing may have led to mouth breathing. My tongue may not have spent enough time in the correct position on my palate, causing a narrower dental arch.
Retractive Orthodontics

I had crowded teeth (small jaws) as a teen, and my upper jaw appeared farther forward than my lower jaw. Instead of correcting my teeth by letting my lower jaw come forward, they pushed my upper jaw back, trapping my lower jaw too far back. This was standard in the 1970s and is known as retractive orthodontics. Teeth were typically moved toward the back of the mouth with the consequence of the tongue having less room to fit in the mouth. As a result, it gets pushed into the throat and blocks the airway. To move my upper jaw back, I was given a special headgear that pushed my top teeth back to meet my lower teeth. As a result, my tongue resided farther back in my throat, causing poor breathing when I slept.
Narrow Dental Arches
The typical distance between the inner cusps of the upper molars used to be greater than 40 millimeters in previous generations. Our arches have been narrowing for the past several hundred years and most of us have less than 35 millimeters today. Airway dentists and orthodontists now expand the arches and bring the jaws forward so that the tongue has more room. Expansion orthodontics also widens the arches, giving the tongue more space.
Sleep Apnea

I have what many orthodontists consider to be a good bite, but I know otherwise. I will show you pictures of my teeth later in this post. The way my teeth fit together is considered Class I or ideal. But my intermolar distance is only 37 millimeters; it should be closer to 40. Additionally, my front teeth overlap too much, trapping my lower jaw farther back than it should be. Both of these problems contribute to a very mild case of sleep apnea.
My Solution: Orthodontic Arch Expansion

Since I have addressed many of the issues that contribute to restriction in my airway; tonsillectomy, adenoidectomy, sinus surgery, correcting my deviated septum, proper sleep hygiene, solid nutrition, low body fat, orofacial myofunctional therapy to make sure my tongue posture is correct, refining my retractive orthodontics was the next step. I am using Invisalign to do this. Invisalign uses clear aligners that are changed out about once per week to move teeth. In addition, they can accurately predict the treatment outcome and simulate it in a short video. We will look at the anticipated results of my treatment shortly.
My Overbite
The amount of overlap of the front teeth is called the overbite. The top teeth should cover no more than 20 to 30% of the lower teeth. As you can see in the photo below, I have straight teeth, but my front teeth overlap my lower teeth by 50%. This forces my jaw back into a retrusive position which can cause airway restriction during sleep, as the tongue can block the throat. The clear aligners can easily change the overlap, and ideal overbite results can be seen in the comparison below.

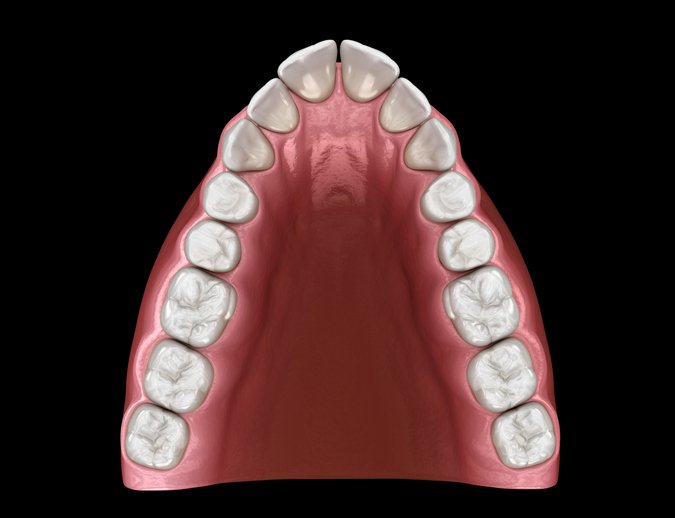
Intermolar Distance
The width of my arch was also too narrow. Studies of skulls from a few hundred years ago all the way back to the stone age show that we all had much wider arches. A typical way to determine the width of the dental arch is by measuring the distance between the inner aspect of the upper first molars. We call this the intermolar distance. Ancestrally, we had widths of 40 plus millimeters. Mine was only 37. My tongue has been crowded out of its proper position. We usually see scalloping on the lateral borders of the tongue with narrow arches. The photos below show the results of my expansion. I went from 37 millimeters to a robust 44 millimeters.

Other Possible Treatments

I was fortunate that my orthodontic treatment only involved clear aligners. However, sometimes other types of expanders are needed when the arches are too narrow. These include fixed and removable appliances. Additionally, surgery can be required for some of the worse cases. The term we use for this is orthognathic surgery. Typically, it involves initial orthodontic movement, followed by the surgery, and then another phase of orthodontic movement to fine-tune everything. If orthodontic treatment is not desired, bite guards and apnea appliances can be fabricated by your dentist.
Conclusion
Hopefully, this post has enlightened you that just because teeth appear straight does not mean all is well. Dentists should be aware of your entire craniofacial respiratory system, which means paying attention to where your jaws are in relation to the rest of your face, especially your nose and pharynx. Dentists also need to consider consulting with various specialists because so many things can negatively influence swallowing, speaking, chewing, and breathing. The specialties include ear, nose, and throat specialists, orofacial myofunctional therapists, allergists, and much more. Lastly, it is never too late to correct growth and development problems.